Table of Contents >> Show >> Hide
- What is knee replacement surgery?
- Why people need knee replacement surgery
- When is it the right time?
- What happens before surgery?
- What happens during knee replacement surgery?
- What are the risks?
- How painful is recovery?
- Physical therapy: the unglamorous hero
- How long does a knee replacement last?
- Life after knee replacement
- Questions to ask your surgeon
- Final thoughts
- Real-life recovery experiences: what people often wish they knew
If your knee has started sounding like a bowl of breakfast cereal and protesting every staircase, you are not alone. Knee replacement surgery is one of the most common orthopedic procedures in the United States, and for many people it can be life-changing. The goal is simple: reduce pain, improve movement, and help you get back to daily life without negotiating peace treaties with your joints.
Still, the phrase knee replacement surgery can feel intimidating. It sounds major because it is major. But it is also a well-established procedure with decades of data behind it. The trick is knowing when it makes sense, what the surgery actually involves, what recovery really looks like, and what questions to ask before you commit. This guide breaks it all down in plain English, minus the medical fog and plus a little honesty about what the process feels like in real life.
What is knee replacement surgery?
Knee replacement surgery, also called knee arthroplasty, is a procedure in which a surgeon removes damaged cartilage and small amounts of bone from the knee joint and replaces them with artificial components. Those components are usually made from metal alloys, high-grade plastic, and other durable materials designed to help the joint glide more smoothly.
Think of it less like getting a brand-new knee from a secret knee warehouse and more like resurfacing a badly worn mechanical hinge. The surgeon is not swapping out your whole leg. Instead, the damaged joint surfaces are reshaped and covered with implants that are meant to restore motion and reduce pain.
Total vs. partial knee replacement
There are two main types of knee replacement:
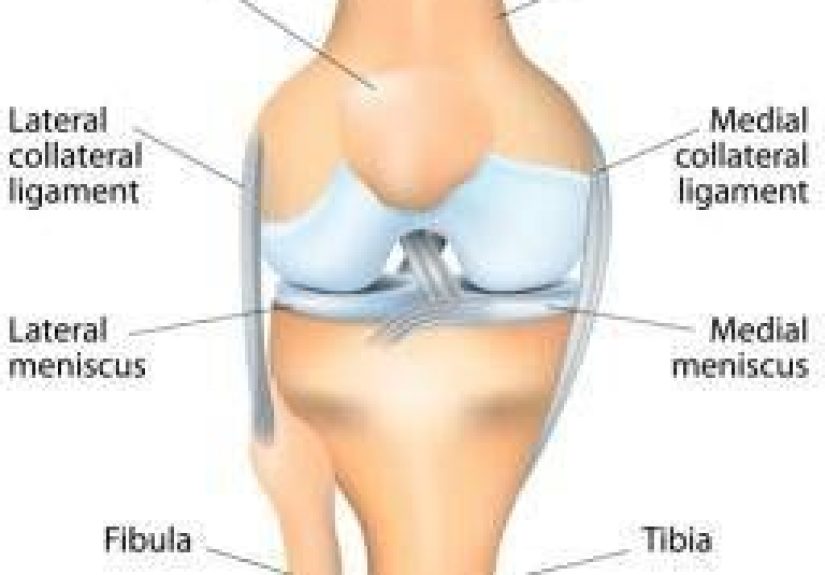
- Total knee replacement: The surgeon replaces the damaged surfaces at the end of the femur, the top of the tibia, and sometimes the back of the kneecap.
- Partial knee replacement: Only the damaged compartment of the knee is replaced. This may be an option if arthritis is limited to one area.
A partial knee replacement can preserve more of your natural bone and tissue, but it is only appropriate for a smaller group of patients. A total knee replacement is more common because many people have damage in multiple parts of the joint.
Why people need knee replacement surgery
The most common reason for knee replacement is osteoarthritis, the wear-and-tear form of arthritis that gradually breaks down cartilage over time. As that cushioning disappears, the bones can rub together, causing pain, swelling, stiffness, and a less-than-lovely grinding sensation.
Other reasons someone might need a knee arthroplasty include rheumatoid arthritis, post-traumatic arthritis after an old injury, certain knee deformities, or severe joint damage that makes walking and daily tasks difficult.
You may be a candidate if you have:
- Chronic knee pain that limits walking, climbing stairs, or getting up from a chair
- Pain at rest or at night
- Stiffness that makes the knee hard to bend or straighten
- Swelling that does not improve reliably
- A knee that has become bowed or knocked inward
- Little relief from medications, injections, braces, physical therapy, exercise programs, or weight management efforts
In other words, knee replacement is usually not the first move. It is more often the “we tried the sensible things first” move. Good surgeons typically want to see that symptoms are serious enough to justify surgery and that less invasive treatments are no longer doing the job.
When is it the right time?
There is no magical age when a person should get a knee replacement. Some people have surgery in their 50s, while others wait until their 70s or 80s. The real question is not your birthday. It is whether your knee pain is shrinking your life.
If you are skipping walks, avoiding travel, waking up at night from pain, or planning your day around where you can sit down next, that matters. If your X-rays look rough but your symptoms are manageable, surgery may not be necessary yet. On the other hand, if your life has gotten noticeably smaller because your knee will not cooperate, it may be time for a serious conversation with an orthopedic surgeon.
This is also why “toughing it out” is not always a badge of honor. Waiting too long can sometimes make recovery harder if you lose muscle strength, mobility, or confidence in walking. The sweet spot is usually when symptoms are clearly affecting quality of life, but you are still healthy enough to recover well.
What happens before surgery?
Preparation for knee replacement surgery starts well before you put on the hospital gown that somehow never closes properly. Your surgeon and care team will usually review your overall health, medications, imaging, and surgical goals. You may need blood work, a physical exam, or clearance from your primary care doctor or specialists.
How to prepare
- Review medications: Some medicines and supplements may need to be stopped before surgery, especially blood thinners.
- Ask about smoking and alcohol: Smoking can slow healing and increase complications, so stopping before surgery can help.
- Strengthen what you can: “Prehab” exercises may improve strength and make recovery smoother.
- Plan your home setup: Clear tripping hazards, arrange a sleeping space if needed, and place essentials within easy reach.
- Arrange support: Even if you are fiercely independent, the first days after surgery are not the ideal time to prove it.
Some hospitals also offer pre-op education classes, and those can be surprisingly helpful. Knowing what is normal after surgery can reduce anxiety and keep every ache from feeling like a five-alarm emergency.
What happens during knee replacement surgery?
On surgery day, you will receive anesthesia, which may be general anesthesia, spinal anesthesia, or a combination with sedation and regional nerve blocks for pain control. The surgeon makes an incision over the knee, moves the kneecap aside, removes damaged cartilage and a small amount of bone, shapes the joint surfaces, and secures the implant components into place.
A plastic spacer is inserted between the metal parts to create a smooth gliding surface. If the underside of the kneecap is damaged, that may be resurfaced too. The incision is then closed, and the real adventure begins: recovery.
Some centers use robotic-assisted knee replacement or computer-guided tools to help with alignment and precision. These technologies can be useful, but they are not magic. The surgeon’s judgment, your anatomy, and appropriate patient selection still matter a great deal.
What are the risks?
Every surgery comes with risks, and knee replacement is no exception. The good news is that serious complications are uncommon, but they are still important to understand before moving forward.
Commonly discussed risks include:
- Blood clots in the leg or lung
- Infection in the incision or around the implant
- Bleeding or wound-healing problems
- Stiffness or limited range of motion
- Implant wear, loosening, or failure over time
- Nerve or blood vessel injury, which is rare
- Pain that improves more slowly than expected
Your surgical team works to lower those risks with antibiotics, blood clot prevention, early walking, physical therapy, and careful follow-up. You also play a part. Following instructions, moving when told to move, and calling your surgeon about warning signs can make a real difference.
Red flags after surgery can include fever, increasing redness, unusual drainage from the incision, calf swelling, chest pain, or shortness of breath. That is not the time for internet detective work. That is the time to call your care team right away.
How painful is recovery?
Let us be adults about this: recovery is not exactly a spa weekend. Most people have pain, swelling, stiffness, fatigue, and a temporary feeling that their leg belongs to someone else. The first few weeks can be challenging. But for many patients, that early discomfort gradually gives way to better function and much less arthritis pain.
Pain management usually includes a combination of medications, ice, elevation, and movement. Many hospitals now use multimodal pain control, which means several strategies are combined to reduce discomfort and limit reliance on opioid pain medicine.
What recovery often looks like
- Day 0 to Day 1: Many patients stand or walk with assistance within hours of surgery.
- First 2 weeks: Swelling, bruising, sleep disruption, and stiffness are common. Exercises matter a lot here.
- Weeks 2 to 6: Walking becomes easier, and many people transition from walker to cane as strength improves.
- Around 6 weeks: Many patients can do more household activities and resume driving if cleared.
- By 3 months: People are often significantly improved, though recovery can continue beyond that.
- Up to a year: Strength, flexibility, and the “this knee finally feels like mine” stage can keep improving.
This timeline varies. A healthy person with strong support at home may bounce back faster. Someone with other medical issues, severe pre-op stiffness, or limited muscle strength may need more time. Recovery is not a race, and comparing yourself to a neighbor who “was golfing in three weeks” is usually unhelpful and occasionally suspicious.
Physical therapy: the unglamorous hero
If the surgeon installs the hardware, physical therapy helps you learn how to use it. After total knee replacement recovery, exercise is not optional decoration. It is part of the treatment.
Therapy focuses on bending and straightening the knee, rebuilding strength in the quadriceps and surrounding muscles, improving balance, and restoring walking mechanics. Walking is important, but it does not replace targeted exercises. Both matter.
This is the part many patients underestimate. The surgery happens in a day. The effort afterward is where a lot of your long-term progress comes from.
How long does a knee replacement last?
Modern implants are durable, but they are not immortal. Many knee replacements last 15 to 20 years or longer, and a large percentage are still functioning well at 15 years. Longevity depends on factors such as age, activity level, body weight, implant design, surgical technique, and whether complications develop over time.
Younger, highly active patients may be more likely to need a revision surgery later in life simply because they put more years of use on the implant. That does not mean younger people should never have surgery. It just means timing should be discussed thoughtfully.
Life after knee replacement
Most people do not get a knee replacement so they can admire X-rays. They get it because they want to do ordinary things again without pain stealing the spotlight. Walking, shopping, traveling, gardening, cooking, and moving around the house are often much easier after recovery.
Low-impact activities such as walking, swimming, cycling, golf, and many fitness routines are commonly encouraged once you heal. High-impact activities like running or jumping sports may be discouraged depending on your surgeon’s guidance and your implant.
It is also normal to notice some clicking, numbness around the incision, stiffness in cold weather, or a knee that feels “different” from a natural one. Better does not always mean identical. For many people, the win is not perfection. It is freedom from constant pain.
Questions to ask your surgeon
- Am I a better candidate for total or partial knee replacement?
- What nonsurgical options are still worth trying?
- What are my personal risk factors for complications?
- Do you expect me to go home the same day or stay overnight?
- What will pain control look like?
- How much physical therapy will I need?
- When can I drive, travel, return to work, and resume exercise?
- What warning signs should make me call your office?
A good knee replacement outcome starts with good questions. If a surgeon explains everything clearly and realistically, that is a very good sign.
Final thoughts
Knee replacement surgery is not a casual tune-up, but it is also not something to fear simply because it sounds big. For the right patient, at the right time, it can reduce severe pain, improve mobility, and restore independence in a way that conservative treatments no longer can.
The best approach is practical, not dramatic. Learn your options, understand the trade-offs, prepare well, and go into surgery with realistic expectations. The first weeks can be tough, yes. But for many people, the payoff is worth it: fewer pain-filled days, easier movement, and a life that no longer revolves around an angry knee.
Real-life recovery experiences: what people often wish they knew
Here is the part many articles rush through: what the experience of knee replacement recovery actually feels like when the hospital bracelets come off and real life shows up. Many patients say the biggest surprise is that the new knee often feels better and worse at the same time in the early weeks. Better because the deep grinding arthritis pain may already be gone or fading. Worse because the knee is swollen, stiff, bruised, and deeply annoyed that someone just did construction work on it.
A common experience is feeling encouraged one day and frustrated the next. On Monday, you may walk farther than expected and feel like a recovery champion. On Tuesday, you may wonder why your knee suddenly feels like a grumpy loaf of bread. That up-and-down pattern is normal. Recovery is rarely a clean upward line. It is more like a staircase with naps.
Sleep is another frequent complaint. Many people expect pain to be the main challenge, but poor sleep often becomes the real villain. Swelling, discomfort, medication schedules, and difficulty finding a comfortable position can make nights feel long. Patients often say they were not fully prepared for how tiring recovery would be, even when things were going well.
Another widely shared experience is the mental side of physical therapy. The exercises themselves may not look dramatic, but doing them consistently takes patience. People often report that bending the knee enough, straightening it fully, and trusting the leg again can feel more emotional than expected. Progress may come in tiny victories: getting into bed more easily, standing up without bracing for pain, or walking to the mailbox without narrating every step.
Many patients also say they wish they had accepted help sooner. Recovery tends to go more smoothly when meals, rides, medication pick-ups, and household chores are not all landing on the person with the fresh surgical knee. Independence is great. So is letting someone else carry the laundry basket for a week.
By the six-week mark, a lot of people start noticing real improvements in day-to-day life. Stairs may still be a work in progress, but walking is often steadier, confidence grows, and the future begins to look less like a rehab schedule and more like normal life. By three months, many patients feel they have turned a meaningful corner, though strength and flexibility can keep improving for much longer.
The most encouraging theme in patient experiences is this: people often go through a stretch where they think, “Why did I do this?” and later arrive at, “I’m so glad I did.” That middle section can be humbling, uncomfortable, and slower than expected. But when surgery is chosen for the right reasons and followed by steady rehab, many patients say the result is not just a better knee. It is a bigger life.