Table of Contents >> Show >> Hide
- What Is Osteoporosis?
- Symptoms: Why It’s Called the “Silent Disease”
- Causes & Risk Factors: How Bones Get Weaker
- Diagnosis & Screening: How Osteoporosis Is Found
- Treatment: What Actually Works
- What Treatment Can Look Like: Two Realistic Examples
- Living With Osteoporosis: Monitoring, Motivation, and Momentum
- FAQ
- Experiences With Osteoporosis: What People Often Notice (and Wish They’d Known)
- Conclusion
Quick heads-up: This article is for education, not a diagnosis. If you’re worried about fractures, sudden back pain, or rapid height loss, a clinician can help you sort out what’s going on.
Osteoporosis is the “quiet roommate” of health problems: it can move in, eat your snacks, and rearrange the furniture (your bones) without making much noiseuntil something snaps. Literally. The tricky part is that osteoporosis often has no obvious symptoms until you have a fracture, so many people find out after a wrist, hip, or spine break that seemed… a little too easy.
The good news: osteoporosis is treatable, and the best plan is usually a mix of smart screening, strength-building habits, fall prevention, and (when needed) medications that reduce fracture risk. Let’s break it downpreferably not your bones.
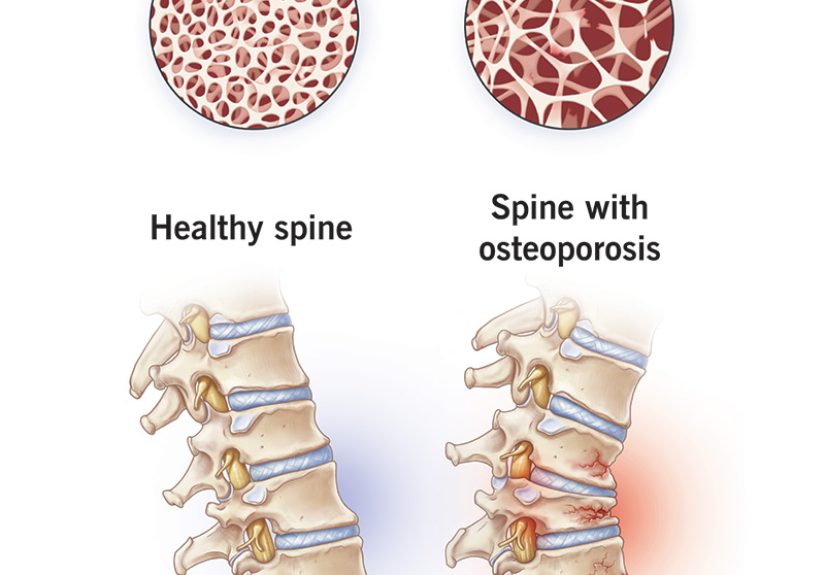
What Is Osteoporosis?
Your bones aren’t dead sticks. They’re living tissue constantly being remodeledold bone is broken down and new bone is built. When the “breakdown crew” works faster than the “construction crew,” bones become less dense and more fragile. That imbalance is the basic storyline behind osteoporosis.
Most people reach peak bone mass around early adulthood. After that, bone breakdown gradually starts to win the tug-of-warespecially after menopause, when estrogen levels drop and bone loss can speed up.
Osteoporosis vs. Osteopenia
Osteopenia means bone density is lower than expected, but not low enough to meet the threshold for osteoporosis. Think of it as a warning lightnot a guaranteed engine failure, but definitely not the moment to ignore your dashboard.
Symptoms: Why It’s Called the “Silent Disease”
Osteoporosis is often symptom-free until a fracture occurs. That’s why screening and risk assessment matter.
Common signs that can show up (often late)
- Fractures from minor falls or seemingly normal activities (bending, lifting, coughing)
- Sudden or severe back pain (sometimes from a vertebral compression fracture)
- Loss of height over time
- Stooped posture or a rounded upper back (kyphosis)
- Shortness of breath in some cases, if spinal changes affect lung capacity
“But I feel finecould I still have it?”
Yes. Many people feel totally normal until the first fracture. If you have risk factors (we’ll cover those next), it’s worth discussing bone density testing with a healthcare professional.
Causes & Risk Factors: How Bones Get Weaker
Osteoporosis usually develops from a blend of age-related changes and risk factors. Some you can’t change, but plenty are modifiablewhich is where prevention and treatment get real traction.
Major non-modifiable risk factors
- Age (risk rises as bone remodeling shifts toward loss)
- Sex (women are at higher risk, especially after menopause; men are still at risk, especially later in life)
- Family history (especially parental hip fracture)
- Body frame (smaller, thinner frames have less bone “reserve”)
Hormonal changes that matter
- Menopause and low estrogen can accelerate bone loss.
- Low testosterone in men can contribute to low bone density.
- Irregular or absent periods in premenopausal women (for example, from certain hormonal or medical conditions) can affect bone health.
Modifiable lifestyle risk factors
- Low physical activity (bones respond to load; they don’t love a sedentary lifestyle)
- Smoking
- Heavy alcohol use
- Low calcium or vitamin D intake over time
- Under-nutrition (including inadequate protein)
Secondary osteoporosis: when another condition (or medication) is the driver
Sometimes osteoporosis is “secondary,” meaning it’s largely caused by another issue. Examples include certain endocrine disorders, gastrointestinal diseases that affect absorption, autoimmune disease, and blood disorders.
Medications can also play a rolemost famously long-term glucocorticoids (steroids). If you need steroids for a chronic condition, don’t panicbut do ask about bone-protection strategies early, not after the first fracture.
Diagnosis & Screening: How Osteoporosis Is Found
Because osteoporosis can be silent, diagnosis relies on risk assessment and testingnot waiting for a dramatic plot twist.
Bone density test (DXA/DEXA)
The most common test is a DXA scan (dual-energy X-ray absorptiometry). It’s quick, noninvasive, and typically measures the hip and spineareas where bone density is especially useful for predicting fracture risk.
T-scores: what the numbers mean
- Normal: T-score of -1.0 and above
- Osteopenia (low bone mass): T-score between -1.0 and -2.5
- Osteoporosis: T-score of -2.5 or lower
Who should consider screening?
Many guidelines recommend screening women at an older age and earlier screening for postmenopausal women with risk factors. Men may also be screened based on individual risk, though recommendations can differ depending on the guideline and the evidence base.
Risk tools: more than a single number
Fracture risk depends on more than bone densityhistory of fractures, age, certain medications, smoking, alcohol, and fall risk all matter. Clinicians often use risk tools plus DXA results to decide whether treatment is recommended.
When your clinician may check for secondary causes
If osteoporosis shows up earlier than expected, progresses quickly, or occurs alongside certain symptoms, clinicians may run labs to look for contributors (for example, vitamin D deficiency, thyroid issues, or other conditions). This is especially important because treating the underlying cause can improve outcomes.
Treatment: What Actually Works
Osteoporosis treatment focuses on two big goals:
- Reduce fracture risk (the main pointbecause fractures change lives)
- Slow bone loss and/or build bone, depending on risk level and medication choice
1) Nutrition: calcium, vitamin D, and “bone-friendly” eating
Bones need building materialsespecially calciumand vitamin D helps your body absorb and use calcium.
How much calcium do you need?
- Adults 19–50: about 1,000 mg/day
- Women 51+: about 1,200 mg/day
- Men 71+: about 1,200 mg/day
How much vitamin D do you need?
- Adults 19–70: about 600 IU/day
- Adults 71+: about 800 IU/day
Food-first is usually the easiest on your stomach and your routine. Calcium-rich options include dairy, fortified plant milks, leafy greens, tofu made with calcium, canned fish with bones, and some fortified cereals. Vitamin D is trickierfatty fish and fortified foods help, and some people need supplements based on levels, diet, sun exposure, or medical conditions.
Important: More is not always better. High-dose supplements can cause problems, so it’s wise to discuss supplement doses with a clinicianespecially if you have kidney disease, a history of kidney stones, or take certain medications.
2) Exercise & safe movement: strengthen bones, muscles, and balance
Exercise won’t “cure” osteoporosis, but it can meaningfully reduce fracture risk by improving strength, posture, coordination, and balance. The best programs usually combine:
- Resistance training (strength work using weights, bands, machines, or bodyweight)
- Weight-bearing activity (walking, stair climbing, dancinganything where your body works against gravity)
- Balance and stability (to reduce falls)
- Posture and core work (especially helpful for spine protection)
If you already have osteoporosisespecially with spine fracturesyour program should avoid sudden, high-impact moves and risky bending/twisting patterns. A physical therapist can help you choose safe exercises that still challenge your muscles (and your bones) without turning your workout into an emergency room cameo.
3) Fall prevention: the most underrated “treatment”
Many fractures happen because of falls, so reducing fall risk is a major part of osteoporosis care. Practical steps include:
- Improve home lighting and use nightlights
- Remove tripping hazards (loose rugs, cords, clutter)
- Use sturdy stepstools with handrails
- Review medications that may cause dizziness or sleepiness
- Update vision prescriptions and consider balance training
- Use supportive footwear and non-slip mats
This isn’t “being paranoid.” It’s being strategic. Think of it as installing guardrails on your health instead of waiting for a crash test.
4) Medications: when lifestyle isn’t enough (and often, it isn’t)
Medication is typically considered when fracture risk is highsuch as a very low T-score, a prior fragility fracture, or elevated fracture risk based on combined factors. The best choice depends on risk level, medical history, kidney function, past fractures, and how urgently bone strength needs support.
Bisphosphonates (often first-line)
These medications slow bone breakdown and have strong evidence for reducing fractures in many high-risk patients. Common examples include alendronate, risedronate, ibandronate, and zoledronic acid (some are pills; some are IV infusions).
Possible side effects include stomach irritation (for some oral forms), flu-like symptoms after IV dosing (for some people), and rare complications like osteonecrosis of the jaw or atypical femur fractures. Rare doesn’t mean “ignore it,” but it does mean decisions should be individualizednot based on scary headlines alone.
Denosumab
Denosumab is an injection that reduces bone breakdown and can be very effective. One key point: if someone stops it, clinicians often plan a transition strategy rather than abruptly discontinuing, to avoid rapid bone loss.
Anabolic (bone-building) therapies
For very high fracture riskespecially multiple fractures or very low bone densityclinicians may consider bone-building medications such as teriparatide or abaloparatide (typically used for a limited duration). These are often followed by an antiresorptive medication to maintain gains.
Romosozumab (sclerostin inhibitor)
Romosozumab can both increase bone formation and reduce bone breakdown. It’s typically reserved for very high-risk cases and is used for a limited time. Because of cardiovascular safety concerns in some patients, it may not be appropriate for people with certain heart or stroke histories.
Hormone-related options (selected cases)
For some postmenopausal womenespecially those who also have menopausal symptomsclinicians may consider menopausal hormone therapy or selective estrogen receptor modulators (like raloxifene) in specific situations, balancing benefits and risks.
Calcitonin (limited role)
Calcitonin is generally reserved for cases where other therapies are not tolerated or appropriate.
What Treatment Can Look Like: Two Realistic Examples
Example 1: The “I shrank an inch” surprise
A 68-year-old notices she’s shorter than she used to be and has intermittent mid-back pain. A DXA scan shows a T-score in the osteoporosis range. Her care plan includes resistance training twice weekly, daily walking, calcium-rich meals, vitamin D based on lab results, home fall-proofing, and a first-line medication to reduce fracture risk. Within months, she reports better balance and confidenceplus fewer “I’m scared to slip” moments.
Example 2: The steroid situation
A 55-year-old has been on long-term prednisone for a chronic inflammatory condition. Even without a fracture, his clinician flags elevated risk and discusses bone density testing, calcium/vitamin D adequacy, strength training, and preventive medication if indicated. The win here is timing: addressing bone health early reduces the chance that the first clue is a fracture.
Living With Osteoporosis: Monitoring, Motivation, and Momentum
Follow-up and monitoring
Bone density changes slowly. Follow-up DXA scans may be spaced out depending on risk level and treatment type. Clinicians also monitor for fractures, side effects, vitamin D status, fall risk, and whether the plan still matches your life (because a plan you can’t follow is just a very detailed wish).
Small habits that add up
- Build “bone moments” into your day: short walks, mini strength sessions, standing balance practice while brushing your teeth.
- Choose protein at meals (muscle supports bonesand helps prevent falls).
- Make your home safer without making it feel like a padded room.
- Ask questions about medstiming, side effects, and how long you’ll likely be on them.
FAQ
Can osteoporosis be reversed?
Some treatments can improve bone density, and many can lower fracture risk substantially. “Reversed” is tricky because fracture risk depends on more than one number, but meaningful improvement is absolutely possible with the right plan.
Is walking enough?
Walking is great and very bone-friendly, but it’s usually not enough by itself for high-risk osteoporosis. Adding resistance training and balance work tends to produce better overall protection.
If I have osteopenia, do I need medication?
Not always. Many people with osteopenia focus on lifestyle and fall prevention. Medication is usually considered when fracture risk is high (for example, based on risk tools, age, or prior fractures). This is a personalized decision.
Experiences With Osteoporosis: What People Often Notice (and Wish They’d Known)
Note: The experiences below are compiled from common patient themes and clinical conversations. They’re not personal medical advicejust the patterns people repeatedly describe when they’re learning to live well with osteoporosis.
1) “I didn’t feel anythinguntil I did.” A lot of people say their diagnosis felt unfair because there weren’t clear warning signs. Some discover osteoporosis after a wrist fracture from a simple slip. Others find out after sudden back pain and a scan showing a vertebral compression fracture. The emotional whiplash is real: one day you’re fine, the next day you’re googling words like “DXA” and “T-score” and wondering whether your spine is secretly made of crackers.
2) The DXA scan anxiety is usually worse than the test. People often worry the scan will hurt or be complicated. In reality, the test is typically quick and painless. What’s stressful is the meaning of the resultsseeing a number that labels your bones as “low” can feel personal, even though it’s just data. Many patients say it helped when their clinician explained the result as a starting point, not a verdict.
3) Medication decisions can feel like choosing between two scary headlines. It’s common to hear, “I’m worried about side effects,” especially with bisphosphonates or injections. People do best when they get a clear, balanced explanation: what the medication helps prevent (fractures), how common side effects actually are, what “rare” means in real life, and what safety steps help (like dental planning, correct pill-taking technique, and regular follow-ups). The biggest relief many report is realizing they’re not committing forevertreatment often includes reassessment points, and the plan can evolve.
4) Strength training feels intimidating… until it feels empowering. Many people start out thinking osteoporosis means they should be extra careful and avoid exercise. Then they learn the real goal is safe loading: resistance training, posture work, and balance practice that makes daily life steadier. A common turning point is noticing practical winsstanding up from a chair more easily, feeling less wobbly on stairs, or simply walking with more confidence. Some even describe strength training as “getting my body back,” because it improves more than bone: it improves independence.
5) Fall-proofing the house is weirdly satisfying. People joke that once they start looking for tripping hazards, they can’t stop. The loose rug gets banished. The dark hallway gets a nightlight. The cluttered stairs get cleared. What begins as a safety project often becomes a quality-of-life upgrade. Several patients describe sleeping better just knowing they’re less likely to fall if they get up at night.
6) Support matters more than willpower. Whether it’s a walking buddy, a physical therapist, a family member helping move furniture, or an online community, people often say osteoporosis became manageable when they stopped treating it like a solo mission. Motivation tends to last longer when it’s attached to something meaningfulplaying with grandkids, traveling without fear, staying independentnot just chasing a “better number.”
If there’s a single theme running through these experiences, it’s this: osteoporosis is common, but helplessness is optional. With the right mix of medical care and daily habits, many people move from “I’m afraid of breaking” to “I know how to protect myself.”
Conclusion
Osteoporosis often stays hidden until a fracture happens, which is exactly why awareness and screening are so important. The most effective treatment plans typically combine nutrition (especially calcium and vitamin D), strength and balance training, fall prevention, andwhen fracture risk is highmedications that meaningfully reduce the risk of broken bones. If you’re at risk or already diagnosed, a clinician can help tailor a plan that’s both evidence-based and realistic for your daily life.