
Table of Contents >> Show >> Hide
- What Osteoporosis Treatment Is Really Trying to Do
- Medications for Osteoporosis
- Home Remedies for Osteoporosis: Helpful, but Not Magical
- Lifestyle Changes That Make Osteoporosis Treatment Work Better
- What a Good Osteoporosis Treatment Plan Looks Like
- When to Talk to a Doctor Sooner Rather Than Later
- What Osteoporosis Treatment Often Feels Like in Real Life: Common Experiences
- Final Thoughts
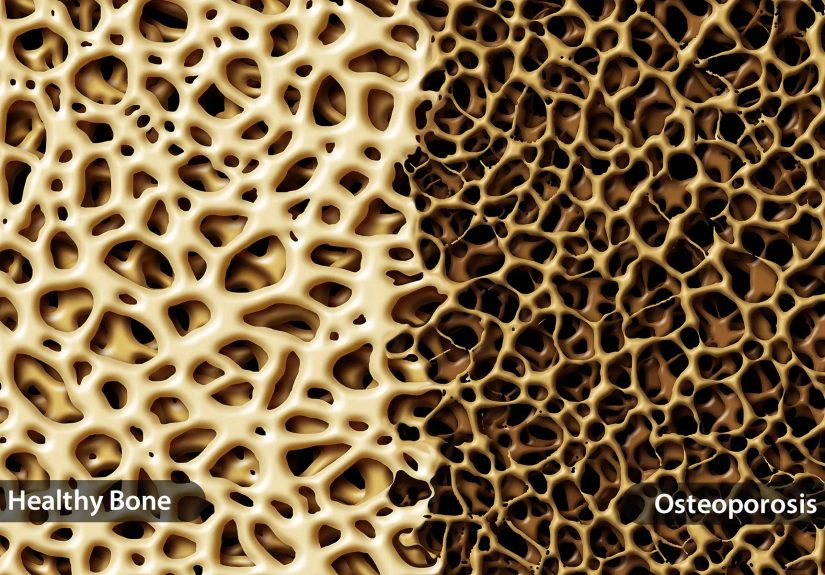
Osteoporosis has a sneaky personality. It does not usually announce itself with fireworks, confetti, or even a strongly worded memo. Instead, it quietly thins your bones until a minor fall, an awkward twist, or an overconfident attempt to lift a suitcase turns into a fracture. That is why treatment matters so much. The goal is not simply to “improve bone density” on paper. The real goal is to keep you strong, mobile, independent, and far less likely to hear the phrase, “Well, that explains the break.”
If you are looking for the best osteoporosis treatments, here is the big picture: there is no single miracle fix. Effective care usually combines the right medication, bone-friendly nutrition, smart movement, fall prevention, and consistent follow-up. Some people need prescription drugs right away. Others benefit most from early lifestyle changes plus monitoring. Most need both. The best plan depends on fracture risk, age, bone density results, medical history, kidney function, and whether a person has already had a fragility fracture.
This guide breaks down osteoporosis medications, home remedies, lifestyle changes, and what real treatment often looks like in everyday life. Consider it your no-nonsense, no-fad, slightly more cheerful roadmap to stronger bones.
What Osteoporosis Treatment Is Really Trying to Do
Osteoporosis treatment is about lowering fracture risk. That sounds obvious, but it matters because treatment decisions are not based on bone density alone. Doctors also look at your history of broken bones, your age, whether you have gone through menopause, family history, medication use, your risk of falling, and sometimes fracture-risk tools such as FRAX.
In practical terms, treatment usually aims to do four things:
- slow down bone loss,
- build new bone when fracture risk is especially high,
- support bone strength with nutrition and movement, and
- prevent falls before they become a very expensive and painful plot twist.
It also helps to remember that osteoporosis treatment is not identical for everyone. A healthy 55-year-old with mild bone loss is not managed the same way as a 78-year-old who already had a hip or spine fracture. Bones, unfortunately, do not believe in one-size-fits-all.
Medications for Osteoporosis
Prescription medications are often the backbone of treatment for people with osteoporosis or a high risk of fracture. Broadly speaking, these drugs fall into two camps: medicines that slow bone breakdown and medicines that help build bone.
1. Bisphosphonates: The Most Common Starting Point
Bisphosphonates are often the first-line treatment for many adults at high risk of fracture. This group includes familiar names such as alendronate, risedronate, ibandronate, and zoledronic acid. Some are taken by mouth on a weekly or monthly schedule. Others are given by IV less often.
Why are they so commonly used? Because they have solid evidence behind them, they are widely available, and they can lower fracture risk in the spine and, depending on the drug, in other major bones as well. For many people, they are the reliable, unglamorous workhorse of osteoporosis care. Not flashy. Very useful.
That said, they are not perfect for everyone. Some oral bisphosphonates can irritate the esophagus or stomach, which is why the dosing instructions matter so much. They usually need to be taken with plain water, first thing in the morning, and followed by staying upright for a period of time. If that sounds like a lot before coffee, you are not wrong.
For some patients, doctors reassess fracture risk after several years of treatment. If risk has dropped to low or moderate, a temporary “drug holiday” may be considered with certain bisphosphonates. That is not a DIY vacation, though. It is a medical decision based on risk and follow-up testing.
2. Denosumab: An Injection That Slows Bone Loss
Denosumab is an injectable antiresorptive medication given every six months. It can be a strong option for people who cannot tolerate oral bisphosphonates, have certain kidney-related treatment considerations, or need another effective way to reduce bone loss.
One important detail: denosumab is not the kind of medication you casually stop because life got busy or your calendar became a disaster zone. Missing, delaying, or stopping it without a transition plan can increase the risk of fractures, especially in the spine. In other words, consistency matters. If denosumab is part of the plan, so is the plan for what comes next.
3. Bone-Building Medicines for Very High Fracture Risk
Some people need more than a medication that simply slows bone loss. If fracture risk is very high, especially after a vertebral fracture or multiple fractures, a doctor may recommend an anabolic or bone-building medicine. These include teriparatide, abaloparatide, and romosozumab.
These drugs are often reserved for people who need a stronger push in the right direction. They help the body form new bone and can be especially useful when osteoporosis is severe. Romosozumab is typically limited to one year of treatment, and teriparatide or abaloparatide are usually used for a defined period before another medication is started to help maintain the gains.
That follow-up step matters. Building bone is terrific, but keeping it is the long game. Without a maintenance strategy afterward, some of the benefit can fade faster than a New Year’s gym resolution.
4. Raloxifene and Hormone-Related Options
Raloxifene is a selective estrogen receptor modulator, often shortened to SERM because medicine loves an acronym. It can be useful in certain postmenopausal women, particularly when spine protection is a major focus. It is not the universal answer, but it may fit the right patient profile.
Hormone therapy can also play a role in some women around menopause, especially when bone protection is considered alongside menopausal symptom relief. But it is not appropriate for everyone, and the decision depends on age, personal risk factors, timing, and broader health goals. This is a conversation for a clinician, not your cousin’s group chat.
5. Calcitonin: Less Common and Usually Not the Star Player
Calcitonin still appears in osteoporosis discussions, but it is generally less effective than the main modern options. It may sometimes be used in select situations, including when short-term pain relief after certain spinal fractures is needed, but it is not usually the first choice when the goal is strong long-term fracture prevention.
Home Remedies for Osteoporosis: Helpful, but Not Magical
The phrase “home remedies” can get a little wild on the internet. Somewhere, someone is probably claiming that one smoothie, three seeds, and a crystal under your pillow can rebuild your skeleton. Realistically, home-based osteoporosis support is far less dramatic and far more effective.
Here are the home remedies that actually deserve attention:
Get Enough Calcium
Calcium is one of the basic building blocks your bones need. Good sources include low-fat dairy, fortified plant milks, fortified orange juice, leafy greens, tofu made with calcium, canned salmon or sardines with bones, and certain fortified cereals. Supplements can help when diet falls short, but many experts prefer food first when possible.
The exact daily amount depends on age and sex, but many older adults need around 1,000 to 1,200 milligrams per day. More is not automatically better. This is bone health, not a competitive sport.
Do Not Forget Vitamin D
Vitamin D helps the body absorb calcium. Without it, your calcium plan is like ordering bricks but forgetting the mortar. Some people get enough through sunlight, diet, and fortified foods, while others need supplements. Adults over 50 are often advised to get roughly 800 to 1,000 IU daily, though individual needs vary and some people need lab-guided treatment.
Eat Enough Protein
Protein is not just for bodybuilders and people who own suspiciously large shaker bottles. Bone is living tissue, and protein helps support muscle and bone health. Good options include fish, eggs, dairy, beans, lentils, soy foods, poultry, and lean meats.
Make Your Home Less Fall-Friendly
This is the one time you want your home to be boring. Remove loose rugs, improve lighting, install grab bars where needed, keep walkways clear, use handrails, and wear shoes with decent traction. Fall prevention is osteoporosis treatment. It may not feel glamorous, but neither is a hip fracture.
Lifestyle Changes That Make Osteoporosis Treatment Work Better
Weight-Bearing Exercise
Walking, dancing, stair climbing, hiking, and low-impact aerobics help stimulate bone. Your skeleton likes gentle, regular reminders that it is still expected to do its job.
Strength Training
Resistance exercise helps build muscle, improve balance, and support bone health. Stronger muscles also reduce fall risk, which is a major win. This does not mean everyone with osteoporosis should immediately start flipping tractor tires. It means structured, safe strengthening matters.
Balance and Flexibility Training
Tai chi, posture work, and targeted balance exercises can reduce fall risk. For many adults, this part is just as important as the bone-density conversation. A person with modest osteoporosis and excellent balance may avoid injuries that a stronger-boned but unsteady person does not.
Quit Smoking
Smoking is bad news for bones. It is associated with lower bone density and higher fracture risk. Stopping smoking helps the whole body, including your skeleton.
Limit Alcohol
Excess alcohol can increase the risk of falling and may contribute to bone loss. Moderate drinking is one thing. Treating your bones like they live in a frat basement is another.
Review Medications and Health Conditions
Some medications, such as long-term glucocorticoids, can worsen bone loss. Certain medical conditions also increase risk. If osteoporosis is on the table, medication review should be too. Sometimes treatment means adding a bone medicine. Sometimes it also means reducing a hidden driver of bone loss.
What a Good Osteoporosis Treatment Plan Looks Like
A strong treatment plan is not just a prescription and a vague instruction to “be careful.” It usually includes:
- a bone density evaluation and fracture-risk assessment,
- a clear decision about whether medication is needed,
- specific calcium, vitamin D, and nutrition goals,
- an exercise plan matched to the person’s ability and fracture risk,
- fall-prevention steps at home, and
- follow-up testing or appointments to see whether the plan is working.
This is important because osteoporosis treatment is not instant. Bone remodeling takes time. Some people expect a dramatic change in how they feel after starting medication, then get disappointed because nothing happens by next Tuesday. The real success metric is usually fewer fractures, steadier bone density, better physical function, and lower risk over time.
When to Talk to a Doctor Sooner Rather Than Later
Call a clinician if you have had a fracture after a minor fall, lost height, developed new back pain, are entering menopause with major risk factors, or have been told you have osteopenia and are wondering whether treatment should start. You should also ask for a review if you are taking steroids long term, have digestive or hormonal conditions that affect bone, or have trouble tolerating an osteoporosis medication.
And yes, men need evaluation too. Osteoporosis is often treated like it only RSVPs to women, but men can absolutely develop it and suffer serious fractures.
What Osteoporosis Treatment Often Feels Like in Real Life: Common Experiences
The lived experience of osteoporosis treatment is usually less dramatic than people fear and more practical than people expect. For many, the journey begins with surprise. Someone goes in for a routine scan after menopause or after a small fracture and hears the word “osteoporosis” for the first time. The first reaction is often anxiety. The second is confusion. The third is usually, “Wait, how did my bones get involved in this?”
One very common experience is learning that treatment is a package deal. A patient may start a weekly bisphosphonate and discover that the real challenge is not the pill itself, but the routine around it. Taking it correctly, staying upright, spacing it away from food and supplements, and remembering the dose every single week can take adjustment. Once it becomes a habit, many people find it manageable. In the beginning, though, it can feel like their medication has more rules than an airline carry-on.
Others learn that the first medication is not always the final medication. A person with stomach irritation may switch from an oral drug to an infusion or injection. Someone with very high fracture risk may start with a bone-building medicine and later transition to a maintenance drug. This can feel frustrating at first, but it is also normal. Osteoporosis care often involves fine-tuning, not failure.
Another common experience is that lifestyle changes start small and then become meaningful. Many people do not transform overnight into kale-chomping, tai-chi-at-sunrise fitness icons. They begin with a daily walk, a protein goal, a calcium-rich breakfast, and a better-lit hallway. Then those simple steps add up. Patients often report feeling more stable, more confident, and less afraid of falling once they start strength and balance work.
There is also an emotional side that does not get enough attention. A prior fracture can make people nervous about movement. Some become overly cautious and start avoiding exercise, which can backfire by weakening muscles and increasing fall risk. With good guidance, many find the sweet spot: safer movement, not less movement. That shift can be powerful. It turns treatment from “protecting fragile bones” into “building a stronger life.”
And perhaps the most honest experience of all is this: osteoporosis treatment rarely feels glamorous. It looks like medication schedules, grocery choices, resistance bands, follow-up scans, and shoes with actual grip. But those ordinary choices can protect independence, reduce pain, and prevent future fractures. In real life, success often does not look dramatic. It looks like gardening without fear, carrying groceries without wobbling, walking with confidence, and staying out of the hospital. For most people, that is a pretty terrific outcome.
Final Thoughts
The best osteoporosis treatments combine science and consistency. Medications can lower fracture risk. Calcium, vitamin D, protein, and exercise help support stronger bones. Fall prevention protects the progress you make. And follow-up keeps the plan aligned with your actual risk, not wishful thinking.
If there is one takeaway worth underlining, highlighting, and sticking on the fridge, it is this: osteoporosis is treatable, and early action matters. Bones may be quiet, but they are not beyond help. Give them the right support, and they usually return the favor.





